by Drs. Jose Ramos-Vara, Peg Miller, ADDL Pathologists, and Dr. Joshua Webster, National Cancer Institute
(The numbers in parentheses correspond to slides with more information, click to view)
Mast cell tumors (MCTs) are one of the most common neoplasms in the skin of dogs, accounting for 7-21% of all cutaneous tumors.3 In the last few years, significant advances in the diagnosis and prognostication of MCTs have been made. This article reviews different aspects of canine MCT, with focus on its classification and the use of immunologic and molecular tools for prognostication.
Three-tier grading versus two-tier grading of cutaneous mast cell tumors. The current grading system of MCTs is based on a
3-tier grading scheme by Patnaik et al,
6 which was designed for dermal mast cell tumors. According to this system, grade 1 MCTs are the least malignant, and more than 90% of dogs survive longer than 1500 days. Neoplastic cells are well-differentiated and confined to the dermis. Mitotic figures are not detected and stromal reaction or necrosis is minimal. Forty-seven percent of dogs with grade 2 (intermediate malignancy) survive longer than 1500 days. Grade 2 MCTs are more cellular than grade 1, have more irregular nuclei, finer cytoplasmic granules and extend into the subcutis. They have low to moderate mitotic index (0-2 mitotic figures/high power field [hpf]). Some contain areas of edema, necrosis or hemorrhage and stromal reaction. Grade 3 MCTs are the most malignant and are characterized by high cellularity, pleomorphic cells with indented to round vesicular nuclei and prominent nucleoli. Grade 3 MCTs typically have 3-6 mitotic figures/hpf and have areas of necrosis, hemorrhage and hyalinized collagen. Only 6% of dogs with grade 3 MCT survive longer than 1500 days. Due to the proven inconsistency among pathologists in grading MCTs based on this 3-tier system, its unsuitability for MCTs confined to the subcutis, and the ambiguity and questionable prognostic value of the intermediate-grade, a new 2-tier grading system
(2) has been developed aand its clinical value is being evaluated.
3 According to this
2-tier grading, a high-grade MCT is one that has any of the following features
(3,4,5,24): at least 7 mitotic figures/10 hpf; at least 3 multinucleated (more than 2 nuclei) cells in 10 hpf; at least 3 bizarre nuclei in 10 hpf; at least 10% karyomegalic cells. Initial results published recently
2 indicate that dogs with high-grade MCTs (using the 2-tier grading system) have significant shorter time to additional tumor development and/or metastasis as well as shorter survival times (less than 4 months for high-grade MCTs versus more than 2 years for low-grade MCTs). This two-tier grading system appears to be more consistently applied by veterinary pathologists than the 3-tier grading system, and at times will be used in the pathology report as a complement to the classic 3-tier (Patnaik) system.
Should I send a biopsy of the regional lymph node from a dog with MCT? In a recent study,1 about 28% of the low-grade (2-tier grading)/grade II (3-tier grading) cutaneous MCTs had metastasized to the regional lymph node. More importantly, none of the cytologic features distinguished low-grade tumors that metastasized from those that did not. The significance of this finding in terms of case outcome is not clear because follow-up information was not available. However, submission of the regional lymph node for histologic evaluation along with the cutaneous biopsy specimen should be considered.
Canine subcutaneous mast cell tumor (SMCT).(9) Most canine MCTs originate in the dermis and eventually extend into the subcutis. These MCTs are termed cutaneous mast cell tumors (CMCTs). However, a proportion of MCTs are localized to the subcutis without a dermal component (SMCTs). The original 3-tier (Patnaik) grading system did not include SMCTs, though the grading scheme has been applied to SMCTs, assuming their behavior is similar to that of CMCTs. Several publications
5,8,9 have identified diagnostic and prognostic differences among CMCTs (those originating from the dermis) and SMCTs (those originating from the subcutis). Based on these studies, it is apparent that most SMCTs have a favorable prognosis, which is supported by extended survival times and fewer recurrences and metastasis when compared with CMCTs. In the study by Thompson et al,
8 SMCTs were classified by a) growth pattern (
circumscribed tumor(10), a well demarcated MCT with expansile behavior;
combined(12), well demarcated solitary nodules of mast cells separated from normal soft tissue by abundant fibrous stroma;
infiltrative tumors(14), similar to combined MCTs but with a distinct infiltrative behavior), b) degree of cellular atypia (anisocytosis and anisokaryosis), c) presence of multinucleated cells, d) cytoplasmic granules, and e) mitotic index (MI), which is the number of mitotic figures per 10 hpf. Results of this study show that SMCTs are rarely fatal (<10% dogs will die of MCT-associated disease), have very low metastatic rate (4%), and low local recurrence (8%) even in those cases with incomplete surgical excision. The estimated 6-month, 1-, 2- and 5-year survival probabilities are 95%, 93%, 92%, and 86%, respectively.
7 Decreased survival time of SMCTs is associated with MI (median survival time for tumors with MI > 4 is 140 days and 950 days for tumors with MI ≤ 4, an infiltrative growth pattern, and presence of multinucleated mast cells.
In summary, if the pathology report states that the MCT is subcutaneous with low MI (≤4), the prognosis is likely to be favorable. As in CMCTs, complete surgical excision (surgical margins free of neoplastic cells) of SMCTs greatly reduces the local recurrence and in many instances adjuvant treatment is not necessary.
Cell proliferation in canine MCTs. Cell proliferation correlates with the outcome of canine MCTs. There are several ways to determine cell proliferation in a diagnostic setting.
- Mitotic index (MI)(24). This is the simplest method to indirectly determine the cell proliferation index. It is performed on conventionally stained (HE) microscopic slides. MI evaluation is done in the area of the tumor with highest mitotic activity. In general, MI correlates with tumor grade and median survival time (MST). In one study,7 dogs with Patnaik’s grade 2 MCT and MI ≤ 5 had a MST of 70 months, whereas those with MI > 5 had a MST of 5 months. Dogs with Patnaik’s grade 3 MCT and a MI ≤ 5 have a MST of more than 6 months, but less than 2 months for those with MI > 5. As mentioned in the previous paragraph, the MI cutoff for canine subcutaneous MCTs is slightly different.
- Ki67 proliferation index(27,28). Ki67 is a nuclear protein that is expressed in all phases of the cell cycle but is not expressed in noncycling cells. The relative number of Ki67-positive cells (detected by immunohistochemical staining) in a tumor constitutes the proliferation index (growth fraction of the tumor). The number of Ki67-positive cells is associated with an increased risk of tumor recurrence at the original site or elsewhere, as well as an increased risk of MCT-related mortality.12
KIT protein expression in canine MCTs. Several mammalian cells including mast cells have a tyrosine kinase KIT receptor, which is encoded by the
c-KIT proto-oncogene. This oncogene is important in normal mast cell survival, proliferation, differentiation, and migration.
12 There are 3 patterns of KIT expression in MCTs: Pattern I
(21) (cytoplasmic membrane); pattern II
(22) (focal to stipple cytoplasmic expression); pattern III
(23) (diffuse cytoplasmic). Several publications have confirmed that increased cytoplasmic expression of KIT protein (patterns II and III) is correlated with increased local recurrence and decreased survival time.
10 Aberrant KIT protein localization (patterns II and III) is also associated with increased cellular proliferation and
c-KIT mutations.
11
c-KIT mutations in canine MCTs. These mutations are most commonly present in the juxtamembrane domain of the receptor KIT, mainly in exon 11 and less commonly in exons 8 and 9, and consist of internal tandem duplications and deletions. c-KIT mutations in canine MCTs are significantly associated with an increased risk of recurrence and death, and a higher tumor grade.11,13 Tyrosine kinase inhibitors are used in the treatment of some canine MCTs with c-kit mutations.
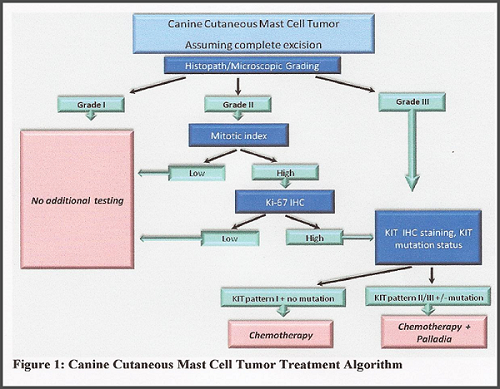 Evaluation of canine MCTs at the Purdue Animal Disease Diagnostic Laboratory. The ADDL offers standard tumor grading of MCTs based on the current grading system, including determination of the mitotic index. When appropriate, we’ll also evaluate MCTs based on the proposed 2-tier grading system as part of the standard biopsy fee. In addition, we offer immunohistochemical evaluation of cell proliferation (Ki67 index) and KIT protein expression. Currently, the ADDL does not perform molecular tests for c-KIT mutations, but we can submit samples to a reference laboratory for that analysis. The main reason for this multi-faceted approach to diagnosis and characterization of various morphologic, immunohistochemical and molecular aspects of canine MCTS is to refine and customize treatment. This approach is summarized in Fig. 1, which depicts a canine cutaneous MCT treatment algorithm followed at the Colorado State University Animal Cancer Center. Keep in mind that other schemes are available and large scale studies are still pending to support this or other approaches to MCT treatment. Our advice is to consult with your oncology service for treatment purposes.
Evaluation of canine MCTs at the Purdue Animal Disease Diagnostic Laboratory. The ADDL offers standard tumor grading of MCTs based on the current grading system, including determination of the mitotic index. When appropriate, we’ll also evaluate MCTs based on the proposed 2-tier grading system as part of the standard biopsy fee. In addition, we offer immunohistochemical evaluation of cell proliferation (Ki67 index) and KIT protein expression. Currently, the ADDL does not perform molecular tests for c-KIT mutations, but we can submit samples to a reference laboratory for that analysis. The main reason for this multi-faceted approach to diagnosis and characterization of various morphologic, immunohistochemical and molecular aspects of canine MCTS is to refine and customize treatment. This approach is summarized in Fig. 1, which depicts a canine cutaneous MCT treatment algorithm followed at the Colorado State University Animal Cancer Center. Keep in mind that other schemes are available and large scale studies are still pending to support this or other approaches to MCT treatment. Our advice is to consult with your oncology service for treatment purposes.
How to be sure that the pathologist is looking at the actual surgical margins?(29) This is one of the most critical points that a pathologist must address in the biopsy report. Regardless of the type of tumor, chances of recurrence are altered by complete (no neoplastic cells in the margins) versus incomplete (presence of neoplastic cells in surgical margins) excision.
2 Tagging different sites of a mass with a suture is a common method to mark margins, but it does not mark the entire surface of the margin (in other words, tagging is good to geographically place a particular area of a mass –cranial, lateral, medial, etc) and does not appear in histologic sections. Therefore, the preferred method is painting of surgical margins
(30,31) (
http://www.addl.purdue.edu/newsletters/2004/winter/tubiop.asp). We prefer dark colors, such as black, blue, and green, to bright shades such as red, yellow or orange, which may fade in histologic processing or be difficult to observe under the microscope. Evaluation of painted margins requires extra technician time and additional sections, which translates into additional cost to the surgical biopsy fee. To paint surgical margins, first blot the surface to be painted, apply the dye, and let it air dry for about 10 minutes before placing it in formalin. Most margins in cutaneous biopsy specimens will be very fatty; to enhance the retention of the dye in adipose tissue, the use of a mordant (e.g., acetic acid) sprayed on the tissue surface before applying the dye is recommended.
By José A. Ramos-Vara1 Margaret A. Miller,1 and Joshua Webster2
1Pathology Section, ADDL, Purdue University, West Lafayette, IN
2Joshua Webster, National Cancer Institute, Bethesda, MD
References:
- Desoutter AV et al (2011) Canine cutaneous mast cell tumor: Correlation between histologic grades and metastasis to regional lymph nodes. Vet Pathol 49:E13 (abstract # 96).
- Kamstock DA et al (2011) Recommended guidelines for submission, trimming, margin evaluation, and reporting of tumor biopsy specimens in veterinary surgical pathology. Vet Pathol 48:19-31.
- Kiupel M et al (2011) Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet Pathol 48:147-155.
- Letard S et al (2008) Gain-of-function mutations in the extracellular domain of KIT are common in canine mast cell tumors. Mol Cancer Res 6:1137-1145.
- Newman SJ et al (2007) Canine subcutaneous mast cell tumor: diagnosis and prognosis. J Comp Pathol 136:231-239.
- Patnaik AK et al (1984) Canine cutaneous mast cell tumor: morphologic grading and survival time in 83 dogs. Vet Pathol 21:469-474.
- Romanski EM et al (2007) Mitotic index is predictive for survival for canine cutaneous mast cell tumors. Vet Pathol 44:335-341.
- Thompson JJ et al (2011) Canine subcutaneous mast cell tumor: Characterization and prognostic indices. Vet Pathol 48:156-168.
- Thompson et al (2011) Canine subcutaneous mast cell tumors: Cellular proliferation and KIT expression as prognostic markers. Vet Pathol 48:169-181.
- Webster J et al (2004) The use of KIT and tryptase expression patterns as prognostic tools for canine mast cell tumors. Vet Pathol 41:371-377.
- Webster JD et al (2006) The role of c-KIT in tumorigenesis: Evaluation in canine cutaneous mast cell tumors. Neoplasia 8:104-111.
- Webster JD et al (2007) Cellular proliferation in canine cutaneous mast cell tumors: Associations with c-KIT and its role in prognostication. Vet Pathol 298-308.
- Zemke D et al (2002) Mutations in the juxtamembrane domain of c-KIT are associated with higher grade mast cell tumors in dogs. Vet Pathol 39:529-535.