Final
Diagnosis: Toxoplasmosis in a juvenile cat
History: A reportedly six to seven-week-old domestic shorthair
cat was submitted to the Animal Disease Diagnostic Laboratory for necropsy.
The history reported that the kitten was found recumbent and nonresponsive in
its cage, and was subsequently euthanized.
Gross findings: Grossly, the cat was in poor body condition and
moderately dehydrated. The thymus was markedly atrophied. Mesenteric lymph
nodes were markedly swollen and bulged on cut section.
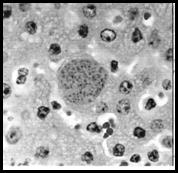
Histologic findings: The hepatic parenchyma contained numerous, variably
sized foci of necrosis. Affected foci contained anuclear and hypereosinophilic
hepatocytes infiltrated by few macrophages and lymphocytes. Few hepatocytes
contained 25-35 µm in diameter protozoal cysts, characterized by a thin cyst
wall containing numerous 1-2 µm in length, punctuate to elongate bradyzoites.
Protozoal organisms were consistent with Toxoplasma gondii tissue
cysts.
|
|
An intrahepatocyte Toxoplasma gondii tissue cyst containing numerous punctuate to crescent-shaped bradyzoites
(H&E, 100X). Note the lack of inflammation surrounding the tissue cyst. |
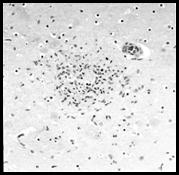
A nodular aggregate of glial cells with
central necrosis within the cerebrum (H&E, 20X). Inflammation is most
likely centered on extracellular tachyzoites. |
The cerebral, cerebellar,
and brainstem parenchyma contained numerous small, nodular foci of necrosis
infiltrated by moderate numbers of glial cells and few macrophages and lymphocytes.
Rare protozoal cysts, not associated with the foci of necrosis, were observed
within the cerebrum.
The adrenal gland
cortices contain multiple foci of necrosis and few intracellular protozoal
cysts.
Mesenteric lymph nodes
contain multiple extensive foci of necrosis.
Pulmonary alveolar septa
were diffusely, markedly expanded by histiocytes and fewer lymphocytes, plasma
cells, and neutrophils. Alveoli were frequently lined by plump epithelial
cells with large round nuclei and few prominent chromocenters (type II pneumocytes)
and contained moderate numbers of histiocytes with abundant eosinophilic,
vacuolated cytoplasm.
Ancillary testing: No bacteria or viruses were isolated by bacterial
culture and virus isolation of the lung, liver, kidney, lymph node, or spleen.
Discussion: The presence of necrosis in multiple organs,
including the liver, adrenal glands, lymph nodes, and brain, along with
protozoal cysts within multiple organs supports a diagnosis of systemic
toxoplasmosis in this cat. Although Toxoplasma gondii and Neospora
caninum are difficult to differentiate histologically, systemic Toxoplasma
gondii infection is by far the most common cause of systemic protozoal disease
in juvenile cats Toxoplasma gondii is an intracellular coccidian
parasite that has a wide host range that includes all domestic species,
rodents, birds, primates, and humans. Domestic cats are the definitive hosts
and the sexual stage of the parasite occurs within feline enterocytes.
Transmission to cats is thought to occur most frequently by ingestion of infected
tissues. Other routes of infection include congenital infection and ingestion
of contaminated feces. Oocysts, which may be shed in the feces of infected
cats, mature into sporozoites, the infectious stage. Once within the host, sporozoites
divide and produce tachyzoites. From the gastrointestinal tract, Toxoplasma is
transported to tissues either free within the plasma, or intracellularly by
lymphocytes, macrophages, and granulocytes. Tachyzoites may infect almost any
host cell to form a parasitophorus vacuole within the host cell membrane.
Proliferation of tachyzoites results in destruction of the host cell and
subsequent release of infectious zoites. These organisms may also encyst
within cells to persist indefinitely as tissue cysts.
The characteristic lesion
associated with systemic toxoplasmosis in cats is necrosis. Lesions may occur
in almost any organ but are most commonly found in the brain, liver, lung,
lymph nodes, heart, skeletal muscle (including the tongue), and eye.
Additionally, a nonsuppurative and proliferative interstitial pneumonia, as was
observed in this case, may occur in disseminated disease.
The majority of infected
cats have clinically silent infection due to an appropriate humoral and
cell-mediated immune response, and subsequent latency of the organism.
Development of systemic disease may be the result of multiple variables
including age, infectious dose, host species, and immune status.
Immunosuppression secondary to stress, glucocorticoids, immunosuppressive
drugs, or viral infection such as FIV, FeLV, and canine distemper virus in
dogs, may predispose the animal to developing systemic disease. Acute
infection of pregnant animals, including women, ewes and does, may result in
parasitemia, placentitis, and abortion or infection of the fetus. Toxoplasma
gondii should be considered as a potential cause of abortion in all
domestic species.
Prenatal or neonatal
infection may result in acute death, or nonspecific signs such as lethargy,
depression, and hypothermia. Other clinical signs include fever, icterus,
neurologic signs, pneumonia, lameness, and ocular abnormalities.
Antemortem diagnosis of
systemic Toxoplasma gondii infection can be extremely difficult.
Serology is frequently used despite obvious shortcomings. A positive antibody
titer indicates exposure but not acute infection, and titers may persist in
latent infection due to the humoral response to tissue cysts. Therefore,
antemortem diagnosis should be based on a combination of history, serologic
testing (preferably acute and convalescent titers) and clinical signs.
-by Dr. Ryan Jennings, ADDL
graduate student
References:
-
Brown CC, Baker DC and Barker IK:
2007. Alimentary system. IN: Jubb, Kennedy and Palmer's Pathology of Domestic
Animals. Ed. Maxie.
-
Dubey JP, Mattix ME and Lipscomb
TP: 1996. Lesions of neonatally induced toxoplasmosis in cats. Veterinary
Pathology 33:290-295.
-
Dubey JP and Lappin MR: 2006.
Toxoplasmosis and Neosporosis. In: Infectious Diseases of the Dog and Cat.
Ed. Greene.
|