Final Diagnosis: Clostridium difficile in a neonatal foal
A 52 kg, reportedly 3-day-old brown Quarterhorse filly was presented with a history of hemorrhagic diarrhea. Other significant clinical findings included metabolic acidosis, gastric reflux, colic, and tachycardia. Abdominal ultrasound revealed dilated loops of intestine. Clinical pathology findings included hypoproteinemia, leucopenia, hypoglycemia, azotemia, hyperbilirubinemia and prolonged partial thromboplastin time. Due to poor response to fluid and antibiotic therapy, the filly was euthanized and presented for necropsy.
At necropsy, the filly was thin and moderately dehydrated. Skin of the lateral abdominal region was shaved bilaterally. The umbilicus was slightly swollen and congested. The abdominal cavity contained about two liters of straw-colored fluid that smelled like urine. Serosal surface of the small intestine (jejunum) along all its length, had multiple, variably sized (up to 5 cm in greatest dimension), oval to irregular depressed areas of necrosis, characterized as central pale tan to gray depressions surrounded by a dark pink to red hyperemic border that sharply demarcated these foci from the normal serosa. A few foci corresponded to mucosal ulcers that were characterized as pale tan to gray depressions on the mucosal surface. The ileum, cecum, and colon contained thick, pale brown to gray fluid. The cecum and large colon had moderate submucosal edema. Well-formed feces were not observed in the small colon and rectum. |
| In the left kidney, there were a few, up to 0.5 cm in greatest dimension, dark pink to red, wedge-shaped foci near the cranial pole that extended into the cortex on cut surface. Both lungs were non-collapsed, wet and heavy, and oozed a moderate amount of pink fluid from the cut surface. Cranioventral portions of the right lung were mottled dark red to pink. A gross diagnosis of mural enteritis with mucosal ulcers and serosal infarcts, abdominal effusions, and pulmonary edema was made. Microscopically, in the small intestine, there was circumferential coagulative necrosis of superficial mucosa (Figures 1,3) Bacterial rods, cocci and coccobacilli were occasionally noted within the necrotic mucosa. The lamina propria was infiltrated by neutrophils, karyorrhectic debris, and hemorrhage.
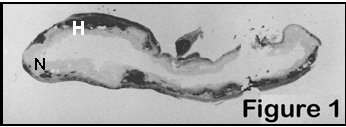 |
Small intestine; foal: Sub-gross view of a section showing diffuse superficial mucosal necrosis (N) and marked hemorrhage in the lamina propria and submucosa (H) |
The submucosa was moderately expanded by edema (Figure 2) and congested blood vessels. A few blood vessels had fibrillar eosinophilic material in their walls and their lumina occluded by partially organized fibrin thrombi. In the colon, there was superficial mucosa necrosis (Figure 4)
|
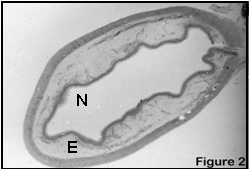
Small intestine; foal: Subgross view of a section showing mucosal necrosis (N) and marked submucosal edema (E) |
|
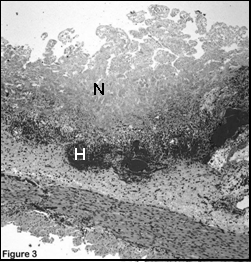
Small intestine; foal: Low power photo-micrograph showing diffuse superficial coagulative necrosis (N) in the mucosa, congestion and peri-vascular hemorrhage (H) |
|
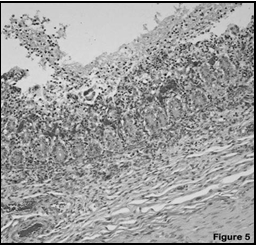
Colon; foal: Low-power photomicrograph showing fibrinonecrotic debris in the superficial mucosa and infiltration by neutrophils and lymphocytes in the lamina propria |
The lamina propria and submucosa were expanded by edema, fibrin, congested capillaries, and increased numbers of lymphocytes and plasma cells. Subserosal connective tissue was expanded by edema, congested blood vessels and infiltration by neutrophils and macrophages, admixed with fibrin and karyorrhectic debris.
Other significant histologic lesions included pulmonary edema and adrenocortical congestion and hemorrhage. Histologic lesions in the small intestine and colon were consistent with a bacterial infection such as salmonellosis and/or clostridial infection. Bacteriological culture of pooled intestinal samples yielded Clostridium difficile, which tested positive for toxin A and B by polymerase chain reaction. Based on acute superficial mucosal necrosis and bacteriological culture, a final diagnosis of C. difficile infection was made. Bacteriological culture for Salmonella sp. was negative.
Clostridium difficile is recognized as an important human and veterinary pathogen, and is an important cause of antibiotic-associated diarrhea in adult humans and various age groups of a variety of animals.
 |
Syrian hamsters, rabbits, pigs, horses, and guinea pigs are most commonly affected. The organism is a gram-positive, anaerobic, spore-forming, rod-shaped bacterium, normally present in low numbers in the intestine of humans, many other mammals, birds and reptiles. Spores are also prevalent in the environment. |
Pathogenic C. difficile elaborates a potent enterotoxin, toxin A, which causes widespread damage to the intestinal mucosa by acting synergistically with a cytotoxin, toxin B. Mucosal damage by toxin A paves the way for the toxin B. Receptors for toxin A are located on the brush border of the enteric epithelial cells. The combined action of these toxins results in necrosis of superficial epithelium and edema in affected areas of intestine. The toxin inactivates Rho and Rho-subtype GTPases in the cytoplasm leading to actin derangements and increased paracellular permeability, cell rounding, and cell death. Additional effects of these toxins include increased production of interleukin 8, which mobilizes and activates neutrophils.
 |
Horses are susceptible to C. difficile infection as adults and foals. Affected adult horses develop necrohemorrhagic typhlocolitis, characterized by superficial mucosal necrosis, hemorrhage and submucosal edema in the cecum and ascending colon. The disease in foals is characterized by severe lesions in the small intestine which include necrohemorrhagic enteritis with severe necrosis of villi, mucosal ulceration and fibrin exudation. Gram positive rods may be observed adhered to the necrotic epithelium. |
Foals can also develop necrotizing colitis similar to adult horses. The disease in foals can develop immediately after birth, responds poorly to therapy, and is usually fatal. The most obvious clinical manifestation of the disease is diarrhea, which may be hemorrhagic. Foals are more susceptible to infection, most likely due to the lack of an established intestinal microflora. Diagnosis is made by bacterial culture, gross lesions and histopathology. Bacteriological culture of C. difficile is not highly sensitive and does not differentiate the pathogenic and non-pathogenic strains. Specific tests for C. difficile toxins used in the diagnostic laboratory include cell culture to detect the presence of biologically active toxin, and an ELISA assay to detect immunologically active toxin that may or may not be biologically active. PCR detection of C. difficile , as was done in this case, is highly sensitive and can discriminate between toxigenic and nontoxigenic strains of the organism by detecting its toxin producing genes. -by Dr. Dinesh Singh, ADDL Graduate Student |