Introduction: Microsporidiosis is a diverse group of diseases caused by microsporidian parasites in a wide range of invertebrate and vertebrate species, including insects, fish, birds and mammals. Traditionally, they were considered protozoa, but recently have been reclassified as fungi based on molecular biology and genomics. These parasites have been reported as causing economic losses in honeybee, fish, mink, and other fur-bearing animals. They also cause problems in the establishment of colonies of specific pathogen free (SPF) laboratory animals for biomedical studies. Nowadays, they are emerging as opportunistic infection parasites in immunocompromised individuals, especially in AIDS patients.
The phylum Microsporidia is subdivided into a variety of families and genera, which includes the genus Encephalitozoon as an important study target,especially for human beings. This genus includes the species E. cuniculi, E. hellem, E. intestinalis and E. lacerate. The latter species was isolated only from reptiles, while the former three species (E. cuniculi, E. hellem, E. intestinalis), together with Enterocytozoon bieneus, were identified as human pathogens. They were reported as causing disease in AIDS patients, organ transplant recipients, children and elderly. Microsporidian spores have been identified in meat and water sources; they are relatively resistant in the environment, and strains of animals were already isolated from humans, raising the concern for the zoonotic potential of microsporidiosis.
In animals, the most common and important pathogen is E. cuniculi. This microorganism is distributed worldwide and present especially in the domestic rabbit population. It may cause different clinical and pathologic presentations, depending on the immune status and species of the affected animal. Although serological studies have been extensively performed and diagnostic tests and treatment have quickly developed during the last few years, further studies are required to completely understand the epidemiology and pathobiology of microsporidiosis.
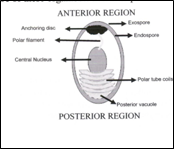
Etiologic agent: Microsporidia are unicellular, spore-forming, obligatory intracellular eukaryotes that are highly resistant to environmental conditions. They characteristically lack obvious mitochondrial structures and have a polar filament, which is a unique feature of these organisms and is important for host cell infection. |
The microsporidian are classified based on the natural host, mode of cell and nuclear division, and ultrastructural features, such as size, nuclear arrangement, number of coils of the polar filament, and developmental stages in the host cell. Typically, Encephalitozoon spp. replicate by binary division within a parasitophorous vacuole, forming 1.5 to 4.0µm, small oval spores containing approximately 4-9 polar filaments coils with single row arrangement. All three Encephalitozoon spp. considered to be human pathogens have morphologically indistinct spores. In the specific case of E. cuniculi, three strains are being recognized based on the animal species from which they were originally isolated and based on the number of 5"GTTT-3" nucleotide sequences: strain I or "rabbit strain", strain II or "mouse strain" and strain III or "dog strain". These have three, two and four 5"-GTTT-3" nucleotide repeats respectively; experimental infection studies failed to prove a host specificity of these strains however.
Life cycle: The life cycle is simple and direct. Most of the infections are acquired through ingestion or inhalation of infective spores, but transplacental transmission of E. cuniculi has also been reported. Rarely, the infection may be transmitted through traumatized epithelium or direct contact. The spore germination occurs when microenvironmental stimuli, such as change in pH or in osmotic pressure, induce posterior vacuole and polarplast alterations, which consequently result in extrusion of the polar filament. This structure is responsible for injecting the sporoplasm into the host cells, which are commonly epithelial cells, macrophages, and endothelial cells. The cycle continues with the development of proliferative forms (meronts) which consequently result in extrusion of the polar filament. This structure is responsible for injecting the sporoplasm into the host cells, which are commonly epithelial cells, macro-phages and endothelial cells. The cycle continues with the development of proliferative forms (meronts), which undergo binary division and differentiate into sporoblasts and sporonts. In Encephalytozoon spp., the cycle occurs within a parsitophorous vacuole (PV) in the host cell, with immature meronts attached to the PV membrane and mature sporonts present in the center. Eventually, the PV and host cell membranes rupture and release spores into the extracellular space. Dissemination may occur by direct extension into adjacent cells or by invasion of the vascular system. The primary sites of infection will depend on the route of transmission, but commonly affected tissues are small intestine, respiratory tract and placenta, with secondary dissemination to kidneys, liver and brain; however, every organ may be affected. The infective spores may be shed through feces, urine or respiratory secretions. This is again dependent on the infection site.
Clinical signs: The clinical signs will depend on the immune status and the species affected, as well as on the pathogenicity of the microsporidian strain. Most of the infected individuals do not become ill and may appear clinically healthy for years. In animals, E. cuniculi is the most important microsporidian pathogen. Serological studies revealed a worldwide range of exposed mammalian species, most of which were asymptomatic. E. cuniculi infection was experimentally reproduced in mice, rabbits and guinea pigs. The clinical signs were worse in immunocompromised animals, such as athymic mice or mice treated with immunosuppressive corticosteroid doses. In rabbits, encephalitozoonosis is a well recognized disease, especially in the domestic rabbit population. Infection probably occurs through ingestion of spores. Occasionally, these animals may develop neurological signs of ataxia, opisthotonos, torticollis, paralysis and head tilt, but more often these clinical signs are a result of bacterial otitis interna. E. cuniculi infection has been described also as fatal infection in newborn puppies and in squirrel monkeys, and as a cause of abortion in horses and non-human primates. In chronically infected dogs, a hyperimmune response may lead to progressive renal failure because of immunocomplex deposition. Severe disease caused by E. cuniculi, characterized by disseminated infection as well as milder clinical presentations such as kerato-conjunctivitis, have been recognized in immune compromised humans. The other pathogenic Encephalitozoon spp., E. hellem and E. intestinalis, are more often associated with persistent diarrhea in AIDS patients and organ transplant recipients.
Pathologic findings: Gross examination commonly fails to demonstrate lesions in cases of encephalito-zoonosis. Usually, the lesions are characterized by lymphoplasmacytic or granulomatous interstitial cell infiltration in multiple sites, particularly in the kidney, liver and brain, but also in the heart, brain, skeletal muscle, and placenta. Especially in immune-compromised hosts, the inflammatory lesions are often accompanied by necrosis and, consequently, by suppurative infiltrate. In fatal cases, these necrotic areas are larger and surrounded by epitheloid macrophages. In cases with chronic liver and kidney involvement, multifocal depressed irregular areas may be present on the renal surface and multifocal pale to yellow areas, characteristic of multifocal hepatitis, may be noted in the parenchyma of the liver grossly. At light microscopy, the organisms may be seen in the center of the necrotic areas; however, parasites may also be visualized without surrounding tissue inflammation, either as small ovoid intracytoplasmatic structures of free within the interstitium. Especially in chronic infections, it may be impossible to find the parasite because it is sparsely distributed and more likely to be disseminated throughout multiple organs. This raises the possibility of underdiagnosis of encephalitozoonosis during routine examination.
Definitive diagnosis and complementary exams: Demonstration of organisms in tissue sections, isolation in tissue culture, inoculation into laboratory animals, electron microscopy, serological tests and molecular techniques such as PCR, are all ways to diagnose encephalitozoonosis. As mentioned above, visualization of the parasite during the histological exam may be difficult in some cases. Gram, periodic acid-Schiff, Warthin-Starry and Giemsa stains have been successfully used to stain microsporidia in tissue sections. Transmission electron microscopy is still the gold standard to identify these organisms based on the detection of the polar filament and PV visualization. Serological exams with determination of antibody titers are useful in epidemiological animal studies and in the control of colonies of SPF laboratory animals. It is important to note, however, that the antigens for such serological assays are available only for microsporidian species maintained in cell culture such as E. cuniculi. Especially when used to evaluate human exposure, the real efficacy of these tests is questionable as there seems to be a risk of nonspecific reaction when spore walls are used as the antigen. More than this, cross reaction may occur, especially in patients with tropical protozoal diseases and, at this time, there are no serological assays that allow the differentiation between current infection and previous exposure to the micro-organism. Efforts are being made to use a recombinant protein of the polar filament as the antigen which gives a highly specific result. The most sensitive diagnostic method to identify microsporidian organisms is still the PCR assay.
Public health importance: Microsporidia are recognized as an emerging opportunistic infectious agent in mammals. The incidence of their diseases is significantly increasing in humans, especially in immunocompromised individuals. Although the most common microsporidium associated with disease in humans in Enterocytozoon bieneusi, Encephalitozoon spp, were also recognized as potential human pathogens. Some authors defend the zoonotic potential of encephalitozoonosis and state that it could occur through exposure of both animals and humans to contaminated water, food or aerosols. The spores are resistant in the environment and can survive for months under humid conditions The chitinous wall of the microorganism seems to be what offers protection against environmental conditions. The identification of microsporidian organisms in water sources is further indicative of a potential waterborne transmission. Nevertheless, additional studies are required to clarify the true risks of waterborne transmission, as well as of other sources of infection such as food and insects. Better characterizations of the biology and epidemiology of these agents may help to determine risk factors, potential therapeutic drugs for humans and animals, and preventive strategies. Veterinarians are fundamental during this process. They work with a wide range of animal species and may therefore be able to conduct comparative biology studies to complement the understanding of microsporidian infection in different hosts.
-by Ana Carolina Maluenda, Extern
-edited by Dr. Inge Langohr, ADDL Graduate Student
References:
-
Didier ES, Didier PJ, Snowden KF, Shadduck JA: 2000. Microsporidiosis in mammals. Microbes Infect 2:709-720.
-
Didier ES, Stovall ME, Green LC, Brindley PJ, Sestak K, Didier PJ: 2004. Epidemiology of microsporidiosis: sources and modes of transmission. Vet Parasitol 126:145-166.
-
Jones TC, Hunt RD, King NW: 1997. Disease due to protozoa. In: Veterinary Pathology, 6th ed., pp 575-578.
-
Juan-Sallé C, Garner MM, Didier ES, Serrato S, Acevedo LD, Ramos-Vara JA, Nordhausen RW, bowers LC, Parás A: 2006. Disseminated encephalitozoonosis in captive, juvenile, cotton-top (Saguinus oedipus) and neonatal emperor (Saginus imperator) tamarins in North America. Vet Pathol 43:438-446.
-
Mathis A, Weber R, Deplazes P: 2005. Zoonotic potential of the Microsporidia. Clin Microb Reviews 18:432-445.
-
Maxie MG, Youssef S: 2007. Nervous system. IN: Jubb, Kennedy and Palmer's Pathology of Domestic Animals, ed Maxie MG, 5th ed. pp 433-435.
-
Patterson-Kane JC, Caplazi P< Rurangirwa F, Tramontin RR, Wolfsdorf K: 2003. Encephalitozoon cuniculi placentitis and abortion in a Quarterhorse mare. J Vet Diag Invest 15:57-59.
-
Tosoni A, Nebuloni M, Ferri A. Bonetto S, Antinori S, Scaglia M, Xiao L, Moura H, Visvesvara GS, Vago L, Costanzi G: 2002. Disseminated microsporidiosis caused by Encephalitozoon cuniculi III (dog type) in an Italian AIDS patient: a retrospective study. Mod Pathol 15:577-583.
-
Visvesvara GS: 2002. In vitro cultivation of microsporidia of clinical importance. Clin Microbiol Rev 15:401-413.
-
Wasson K, Peper RL:2000. Mammalian microsporidiosis. Vet Pathol 37:113-128.
|