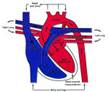
The ductus arteriosis is the fetal connection between the descending aorta and the main
pulmonary artery, allowing the shunting of fetal oxygenated placental blood from the pulmonary artery
to the systemic circulation bypassing the atelectic non-functional fetal lung. Following parturition and the onset of breathing, the rapid increase in arterial oxygen
tension causes constriction of ductal smooth muscle and functional closure of the ductus. Anatomic
obliteration occurs by necrosis and fibrosis during the first few weeks of life. Patency of the ductus
arteriosus beyond 7-10 days of age is considered abnormal in dogs.
Failure of ductal closure appears to be the result of histologic abnormalities within the
ductal wall. The normal ductal wall contains a loose branching pattern of circumferential smooth muscle throughout its length.
In prenatal pups bred to have a high probability of PDA, varying portions of the ductal wall
resemble the wall of the aorta, lacking constricting smooth muscle.
The anatomic appearance of the patent ductus is varied. There is a progression from a
ductus diverticulum that is a blind, funnel-shaped outpouching of the aorta at the site of ductus,
to a ductus that approaches the size of the aorta. The length and diameter of the ductus also vary. In some cases, there is virtually no ductus but, instead, an opening between the aorta and pulmonary artery.
Left to right Patent Ductus Arteriosus:
Left to right is the typical form of PDA in which the aortic pressure is higher than pulmonary artery pressure
throughout the cardiac cycle, and blood shunts continuously from the aorta to the pulmonary
artery. This results in a continuous cardiac murmur, increased pulmonary flow, volume
overloading, and diastolic dilatation of the left atrium and left ventricle. The left
ventricle also undergoes eccentric hypertrophy and increased left ventricular end-diastolic
pressure. If the defect is wide enough to allow a large shunt and pulmonary vascular
resistance remains low, the end result may be left ventricular failure with pulmonary edema.
Left ventricular stroke volume is increased (Frank-Starling principle) and is reflected in an
increased arterial systolic pressure.
In addition, rapid run-off blood from the aorta via the ductus causes a decreased
aortic and arterial diastolic pressure. The wide arterial pulse pressure is felt as a bounding,
hyperkinetic arterial pulse. Increased volume flow in the aortic arch and pulmonary artery
causes dilatation of the aorta and main pulmonary artery. The right ventricle never handles
the shunted blood and remains normal unless there are increases in pulmonary vascular resistance
and pulmonary arterial pressure. Experiments in dogs involving aortopulmonary ducts indicate
that a communication of 3 mm or less in diameter may lead to the slow development of left
ventricular hypertrophy, but it is otherwise well tolerated. A shunt of 5 mm diameter may
lead to pulmonary hypertension, with degenerative changes in pulmonary vessels and congestive
heart failure. When the pulmonary artery resistance increases, right- to-left, or reverse,
shunting PDA develops; this condition will be described later in this article.
Clinical signs rarely develop within the first week of life, and many diagnoses are made at
the time of initial examination at 6-8 weeks or later. In all but the mildest cases with very
small shunts, arterial pulse is hyperkinetic (bounding). Mucous membranes are pink in the
absence of heart failure. A continuous trill may be palpated at the heart base and a
continuous murmur is audible at the same point.
Noninvasive studies are usually diagnostic. Electrocardiography usually indicates left
ventricular enlargement by a normal frontal plane QRS axis and increased R-waves in leads
II, III, Vf, V2 and V4. Left atrial enlargement may also be indicated by widening of P waves.
Radiography demonstrates cardiomegaly, pulmonary hyper-vascularity, left atrial and ventricular
enlargement. The most specific finding is the appearance of an aortic bulge near the origin of
the ductus. The diagnosis could be proved by echocardiography in almost all cases. Ductus
diverticulum, a hidden form of PDA, can be diagnosed only by angiography or necropsy.
Approximately 64% of the dogs diagnosed with left-to-right shunting PDA will die from
complications within a year of diagnosis without surgical correction. Some dogs with modest
shunts will survive to maturity, and a few may live 10 years or more.
Right-to-left Patent Ductus Arteriosus
Right-to-left, or reverse, shunting PDA occurs when there is an increase in pulmonary
vasculature. Dogs with reverse PDA exhibit diminished pulmonary flow, a comparatively small
left ventricle, and marked hypertrophy of the right ventricle. The exact mechanism by which
the pulmonary vasculature resistance increases is not completely understood, but anatomic
description of the pulmonary microvasculature is similar for both humans and animals.
Histologic changes within small pulmonary arteries include hypertrophy of the media, thickening
of the intima, reduction of lumen dimensions, and plexiform lesions of the vessel wall.
Most of these changes are considered irreversible.
Many owners do not recognize obvious clinical signs in their pet during the first 6-12
months of life. Clinical examination is very different from the more common left-to-right PDA.
Physical examination reveals either no murmur or only a soft, early systolic murmur at the
left heart base. Differential cyanosis (cyanosis of the caudal mucous membranes with pink
cranial membranes) may be observed, but recognition may require examination after exercise.
Differential cyanosis is caused by the location of the PDA, which shunts right to left from
the pulmonary artery into the descending aorta. Perfusion of the kidneys with hypoxemic blood
leads to secondary polycythemia and hyperviscosity,
with the PCV gradually increasing to 65% or greater. Polycythemia may occur during the first
year but often does not become severe until 18-24 months of age, therefore, many times
owners do not recognize clinical signs until the condition has progressed.
The electrocardiogram shows changes of right hypertrophy. Thoracic radiographs and
echocardiography demonstrate right ventricular hypertrophy and a dilated main pulmonary artery.
Animals with reversed PDA often live 3-5 years; a few survive beyond 7 years if the PCV is
kept below 65%.
Summary: Left to right shunting Patent Ductus Arteriosus is the most common
congenital heart disease in dogs and is caused by failure of ductal closure after birth.
Almost all affected dogs will die from complications before maturity if the
condition is not treated. After surgical treatment, the prognosis is excellent.
Right to left Patent Ductus Arteriosus occurs when there is an increase in pulmonary
vasculature pressure and is an uncommon condition.
-by Horia Popa, ECFVG Student
-edited by Dr. Alok Sharma, ADDL Graduate Student
References:
- Fox, PR. Canine and Feline Cardiology.
- Jubb KVF, Kennedy PC, Palmer N: Pathology of Domestic Animals, 3rd ed.
- Merck Veterinary Manual, 8th ed.
- School of Veterinary Medicine, Purdue University
- Siems J: Radiographic Recognition of Common CongenitalCardiac Disorders in the Dog.
- Textbook of Veterinary Internal Medicine. Ettinger SJ, Felman EC, eds.
|