Swine Influenza
Influenza virus infections are not only an important and common cause of respiratory disease to pigs across the world, but also pose important human public health concerns. Swine influenza virus first appeared in western Illinois in 1918, where it caused not only an epizootic outbreak in swine, but also a pandemic in humans. There is definitive evidence that influenza virus can spread betweenspecies including swine, chickens, ducks, turkeys, wild birds, and humans. With the recent interest in avian influenza, it is important tounderstand that pigs can be “mixing vessels” for the various strains of influenza because they are susceptible to infection with both human and avian influenza A viruses. Their ability to become co-infected with various strains can lead to geneticreassortment of the virus and several different types of viral reassortments have been isolated from pigs around the world, especially from China and the Far East. This poses an important public health concern since swine could serve as a host to create novel mammalian influenza viruses that could lead to a pandemic outbreak in humans. This article will discuss the important features of swine influenza virus,including etiology, epidemiology, clinical signs, lesions, diagnosis, and prevention.
Swine influenza is an influenza A virus in the family Orthomyxoviridae. They are pleomorphic enveloped viruses. Since the virus has a lipid envelope, it is very susceptible to detergents and many common antiviral disinfectants. The influenza virus can easily undergo genetic reassortment due to their segmentedgenome. Influenza viruses are named based on the major surface antigens. There are 13 hemagglutinins (H) and 9 neuraminidase (N). The two major subtypes affecting pigs in the U.S. are H1N1 and H3N2. H1N1 is the classic subtype in swine and has been the predominant strain in the U.S. since 1918. Theemergence of H3N2 occurred in 1997 and is now commonly isolated as well.
In the United States today, swine influenza is common and widespread, with serologic surveys of the Midwest revealing that nearly all herds have antibodies to the virus. Swine influenza can occur in all ages of swine. Historically, acute seasonal outbreaks in the fall and early winter months were most commonly recognized. Today, due to an increase in confinement operations, endemic swine flu causes continuous low levels of disease year round in many swine herds. Influenza virus is most commonly transmitted through pig-to-pig nasal contact since the virus is shed in nasal secretions. Also, the virus can be introduced into a herd during movement of new animals.
The incubation period for swine influenza virus ranges
from 1-3 days, with viral shedding as early as 1 day post infection and ceasing within 7 days. Even though swine influenza is an acute infection and cleared rapidly, clinical illness can persist for weeks in a herd, while the virus is being transmitted from pig to pig. The severity and course of infection depends on co-infection with other agents, age, and overall immune status. The virus usually replicates in the nasalepithelium, lungs, trachea,, tonsils, and tracheo-bronchial lymph nodes, most commonly limiting the viral infection to the respiratory tract. The viral attachment and replication in the nasal and trachealepithelium damages the mucociliary apparatus which allows the infection to spread to the lungs. This can then predispose the pig to secondary bacterial infections in the lung.
The diagnosis can be made presumptively based on clinical signs. The clinical signs of a typical outbreak include pyrexia, anorexia, lethargy, prostration, huddling, and reluctance to move. Nasal and ocular discharge may also be observed. A characteristic dry, hacking “goose honk” cough may also be heard and is associated with the animals being forced to move. The disease may progress to open mouth labored breathing. In uncomplicated swine influenza infections, there is high morbidity and low mortality, causing loss of body condition, weight loss, and delays in marketing (about 1 week). Recovery begins about the 6th day post infection and the herd is generally recovered in a week or two. If clinical cases of swine influenzabecome complicated with other pathogens such as Actinobacillus pleuropneumonia, Pasteurella multocida, Mycoplasma hyuopneumoniae, or Streptococcus suis, this can increase mortality or prolong recovery time. Subclinical infections do occur in finishing pigs. Reproductive problems, such as abortion or small, weak litters, have been associated with acute illness in swine influenza in sows.
Gross lesions associated with uncomplicated swine influenza are typical of viral pneumonia. The lungs are red, wet and heavy. The lesions are often more severe in the apical and cardiac lung lobes, and typically include a patchy or checkerboard pattern of distinct purple collapsed lobules (bronchointerstitial pneumonia). Some blood tinged fibrinous exudate may also be observed in the airways, and the associated bronchial and mediastinal lymph nodes may be enlarged.
The common histopathologic lesion of swine influenza infection is attenuation, necrosis, and desquamation of the bronchial and bronchiolar epithelium. The airway lumens are often plugged with neutrophils, monocytes, and necrotic epithelial cells. Alveolar septae arethickened with lymphocyte, macrophage, and plasma cell infiltrates, and may have type-2 pneumocyte hyperplasia. There is also peribronchial and perivascular cuffing by lymphocytes.
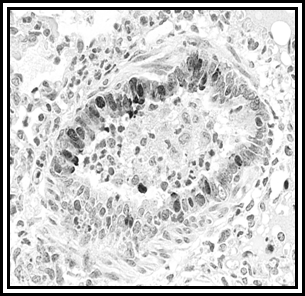
Definitive diagnosis is based on virus isolation from a swab of nasal mucosa or pharynx, for very young pigs. The swab should be made of polyester, not cotton, and should be kept cold during transport. The virus is best isolated from the nasal and pharyngeal secretions when the animals are febrile. Diagnosis can also be done by immunohistochemistry (IHC, Fig. 1&2)
|
Figures 1&2: IHC images are representative of immunostaining of the viral antigen, which is present in the cytoplasm and/or nucleus of the bronchiolar epithelium. Photos are courtesy of Dr. Jose Ramos-Vara
Since there are no specific treatments for swine influenza infections, prevention and control are very important. Treatment of clinically ill animals can include anti-inflammatories to offer some relief for the severely affected, antimicrobials to prevent secondary bacterial infections and, most importantly, clean fresh water, good management and environment.Prevention is largely dependent on biosecurity and avoiding the introduction of carrier animals. New animals to be introduced into the herd can be vaccinated while in isolation and acclimation. Inactivated swine influenza vaccines are commercially available. All ages of swine may be vaccinated and immunity lasts about three months. Colostral immunity will interfere with vaccination in pigs <10-13 weeks old. Influenza control in nursing pigs can be achieved by vaccinating the sow five and two weeks pre-farrowing, which will increase maternal antibody levels. Successful control of swine influenza in the grower/finisher phase of swine influenza positive herds can be challenging. To control influenza during this phase, pigs can be vaccinated at ten weeks of age, and then again two weeks later.
-by Angie Delks, PUSVM Class of 2008
-edited by Dr. Duane Murphy, Heeke ADDL
References:
-
Amass, Sandra. VCS 510. Swine Medicine class notes. Fall 2005-2006.
-
Cos NJ and Subbarao K: 2000. Global Epidemiology of Influenza: Past and Present. Annual Review of Medicine. 51: 407-421.
-
Schwartz KJ: 2004. Swine Disease Manual, 4th ed. American Assoication of Swine Veterinarians.
-
Straw B et al (eds): 2006. Diseases of Swine, 9th ed. Blackwell Publishing, Ames, IA.
|