FINAL DIAGNOSIS: Bovine Anaplasmosis
Case #1
History: In October, 2004, two mature crossbred beef cows, from a herd of 30 cows, were submitted for diagnostic necropsy. The first cow was a 1000 lb white Charolais-cross which was reportedly 14 years old, and had a history of "suddenly going crazy". Because of her unpredictably aggressive behavior, the farmer used his tractor to separate her from the herd, but the cow charged the tractor head first, fell over, and died shortly after the impact. The second cow was a 950 lb red-and-white Hereford cross which was reportedly 10 years old. This cow had been vaguely lethargic for about 24 hours, followed by sudden death. No clinical symptoms had been observed in the remaining 28 cows.
Gross findings: The gross lesions were similar in both cows, though the carcass of the second cow was markedly autolytic at the time of submission. Both were in good flesh and had adequate to abundant body fat. The serosal surfaces of the abdominal organs had a slight yellow discoloration (mild icterus) and the spleens were markedly enlarged (splenomegaly), dark red in color, and bulged from the cut surface (congestion). The spleen of the first cow weighed 2.1 kg (0.46% of her body weight) and the spleen of the second cow weighed 2.5 kg (0.6% of her body weight.) Normal splenic weight for a cow is 0.17% of body weight. In addition to the mild icterus and marked splenomegaly, the first cow had subcutaneous hemorrhage (bruising) on the forehead, while the second cow had a gravid uterus containing a 21cm male fetus. Other than the subcutaneous hemorrhage, there were no fractures or other traumatic lesions that would account for the death of the first cow.
Histopathologic findings: Because of the aberrant neurological behavior, the brains of both cows were examined histologically. No lesions were found. Other tissues were not examined, but expected histologic lesions would be mild. The liver would be expected to have centrilobular degeneration and necrosis secondary to anemic hypoxia. The spleen would have been congested.
Other laboratory findings: Postmortem pericardial fluid from the first cow was positive for Anaplasma antibodies by the ELISA test. Blood smears were not available for examination. Tests for rabies virus and BSE were negative. No bacteria were isolated from spleen, and no viruses were isolated from spleen and lung.
Final diagnosis: Anaplasmosis was diagnosed on the basis of history, compatible gross lesions, and serology.
Follow-up analysis: The referring veterinarian submitted blood samples from nine other cows in this herd; seven of the nine were serologically positive for anaplasmosis by the ELISA test.
Case #2
History: At approximately the same time, a 900 lb, reported nine-year-old Angus cow from a different farm in a different county was submitted for diagnostic necropsy with a one-two day history of vague lethargy and anorexia terminating in sudden death. This cow reportedly came from a herd of about 30 cows from which 6 had died in the past week with similar clinical signs.
Gross findings: The submitted cow was in fair to thin body condition, with very little body fat. Mucous membranes and serosal surfaces had a slight yellow discoloration (slight icterus). The spleen was markedly enlarged (1.7 kg, 0.42% of body weight) and congested. Feces were dry and hard. No other remarkable gross lesions were present.
Other laboratory findings: A sample of postmortem body fluid was serologically positive for Anaplasma by the ELISA test. No viruses were isolated from lung or spleen.
Final diagnosis: Anaplasmosis was diagnosed on the basis of history, compatible gross lesions, and serology.
Follow-up analysis: The referring veterinarian went to observe the herd and reported that the outbreak looked like anaplasmosis, with several cows in the herd exhibiting weakness, anemia, and jaundice. Serum was collected from one of these cows and submitted for serology; it was found to be positive for anaplasmosis by the ELISA test.
Retrospective study: Purdue ADDL records were searched for all cases to which a pathologist had assigned the diagnosis of 'anaplasmosis'. Records searched were from a five year period extending from July 2000 to June, 2005. In that time period, anaplasmosis was diagnosed in 13 different submissions representing 11 different outbreaks (average of 2.6 submissions/year). All submissions were from the southern third of Indiana, with 4 from Jefferson County, 2 from Harrison County, 2 from Lawrence County, and one each from Orange, Perry, Clark, Switzerland and Franklin Counties. All cases were submitted during the months of August (1 case), September (5 cases), or October (7 cases) The age of the affected cattle ranged from 3-14 years, with a median age of 7.5 years. The most common clinical history was sudden death (7 cases), but several had a history of sudden aggression progressing to death in 1-2 days (3 cases) or vague lethargy progressing to death in 1-2 days (3 cases).
Discussion: Although anaplasmosis is not a common disease, it does occur in southern Indiana and is diagnosed on a fairly regular basis. Based upon conversations with experienced practitioners, anaplasmosis has been present in southern Indiana for as long as can be recalled. Because the signs and lesions of anaplasmosis can be subtle, its diagnosis is often missed if the practitioner is not already familiar with the disease. One practitioner commented that he never "saw" anaplasmosis until ADDL had diagnosed a case for him. He then realized he had been seeing it for years without recognizing it. After that, he diagnosed it much more frequently.
The cause of anaplasmosis is Anaplasma marginale, a rickettsia-like organism that is an obligate parasite of bovine red blood cells. The same organism can cause subclinical infections in sheep, goats, whitetail deer, and other ruminants, but the role that these other species might play in maintaining and spreading the disease is unknown. A related organism, Anaplasma ovis, causes clinical anaplasmosis in sheep and goats. Anaplasmosis is spread by the transfer of infected blood via ticks, biting flies and gnats, castration tools, hypodermic needles, etc. Ticks are the most important vector, as some species are biological vectors, maintaining the infection for long periods of time. Species of ticks believed to serve as vectors for anaplasmosis include Dermacenter andersoni, Dermacenter variabilis, Boophilus annalatus, Boophilus microplus, and Argas persicus. Dermacenter variabilis is common in Indiana and may be the vector in southern Indiana. The incubation period after an infective tick bite is believed to be about 1-3 months.
Morbidity and mortality can vary greatly. In my experience, anaplasmosis usually presents as sporadic death loss, affecting only one or a few animals in a herd. But occasionally, as in the second case presented above, it can affect a large number of animals. This may depend upon the herd's prior exposure to the organism. Recovered or latently infected animals are believed to be fairly resistant to the clinical disease, whereas naïve animals are believed to be highly susceptible. Animals that survive infection or that are subclinically infected are believed to maintain a low level of infection throughout life and can serve as a source of infection to other animals. Interestingly, young animals seem to be quite resistant to the disease, and I have never seen a clinical case in an animal less than three years of age. Young animals, however, do easily acquire subclinical latent infections. There is some thought that latently infected animals may become clinically diseased later in life if they experience some kind of physiologic stress such as poor nutrition or other disease.
The primary effect of the infection is to induce extravascular hemolytic anemia, and anemia is presumed to be the cause of death. The clinical signs and lesions of anaplasmosis can be subtle, but if affected animals are examined closely, they will be found to be anemic and may have mild icterus. In the acute phase of infection, animals will be febrile. Aggression and excitability are often reported in affected animals. The cause for this aggression is not known, but it is presumed to be due to the effects of hypoxia on the brain. Postmortem lesions in the dead animal are often mild. In my experience, the most useful postmortem lesions are anemia combined with marked splenic enlargement and congestion. Assessment of splenic size is sometimes difficult for those who do not necropsy many cattle, particularly if the carcass has become autolytic and the spleen has become artifactually inflated with postmortem emphysema. In this case, it is useful to weigh the spleen and compare it to the body weight of the cow. In the normal cow, the spleen should account for 0.17% of the normal body weight. If the spleen is more than twice this weight, it can be determined with confidence that the spleen is enlarged.
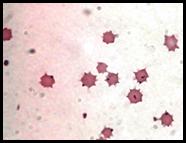
It is difficult to confirm a diagnosis of anaplasmosis from a dead animal, as Anaplasma marginale cannot be cultured. If body bluid or serum can be collected, it can be submitted for serology. It is probably better to closely examine the remaining herdmates, looking for an animal that is febrile, anemic, and/or icteric, and collect serum and unclotted blood from that animal. A CBC should have changes typical of regenerative hemolytic anemia and Anaplasma organisms may be seen at the margins of red blood cells. However, the organisms are not always easily found and it is often necessary to submit serum for serologic testing to confirm the diagnosis.
Animals affected by anaplasmosis can be treated with tetracycline. Penicillin, cephalosporins, and related antibiotics are not effective. A good clinical reference manual should be consulted for more detailed treatment information.
-by Dr. Duane Murphy, ADDL Pathologist
References:
-
Jubb, Kennedy and Palmer: 1991. Pathology of Domestic Animals, 4th ed. Academic Press, Inc., New York, NY
-
Timoney, Gillespie, Scott, Barlough: 1988. Hagan and Bruner''s Microbiology and Infectious Diseases of Domestic Animals, 8th ed., Comstock Publishing Assoc., Ithaca, NY.
-
Blood, Radostitis, Henderson: 1983. Veterinary Medicine, 6th ed., Bailliere Tindall, Philadelphia, PA.