Thus, major mechanisms for triggering DIC include release of tissue factor or thrombo-plastic substances into the circulation (activation of extrinsic pathway of coagulation), injury to endothelial cells exposing subendothelial collagen (activation of intrinsic and extrinsic pathways of coagulation), systemic hypercoagulopathy (renal disease with loss of antithrombin III) and hepatic disease (decreased synthesis of coagulation factors and anticoagulants). Release of tissue factor and/or thromboplastic substances in the circulation is often triggered by sepsis, severe tissue destruction (trauma, burns), pancreatitis, neoplasms (mucinous carcinomas, leukemia, lymphoma, hemangiosarcoma) and/or obstetric complications. Endothelial injury can initiate DIC by release of tissue factor and promoting platelet aggregation to exposed collagen. Causes of endothelial injury include vasculitis due to deposition of antigen-antibody complexes (lupus erythematosus, feline infectious peritonitis), temperature extremes (heat stroke, burns) and/or direct damage by trauma, toxins, rickettsiae, bacteria, or their toxins and/or viruses.
Endotoxemia (gram negative sepsis, intestinal infarction) is one of the most important and often fatal causes of DIC. In macrophages and monocytes, bacterial endotoxins stimulate increased synthesis and release of tissue factor and the proinflammatory mediators interleukin 1 (IL1) and TNFα, which in turn induce procoagulatory functions of endothelial cells such as increased expression of tissue factor and decreased expression of thrombomodulin. In addition, TNFα also upregulates expression of adhesion molecules on endothelial cells and, thus, promotes adhesion of leukocytes which may damage endothelial cells by release of proteolytic enzymes and oxygen-derived free radicals. Bacterial endotoxins can also directly activate factor XII.
Mucus released from some carcinomas acts as thromboplastic substance and directly activates factor X and, thus, is the common pathway of coagulation. In acute promyelocytic leukemia, granules of neoplastic leukocytes release thrombo-plastic substances. Tissue destruction (trauma, burns) causes release of thromboplastin in circulation. Release of proteolytic enzymes in the circulation and thus marked tissue destruction, is caused by pancreatitis. Thromboplastins derived from placenta, dead fetus and/or amniotic fluid may enter the maternal circulation in obstetric complications.
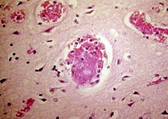
Activation of intravascular coagulation is followed by formation of thrombi within the microcirculation of multiple organs such as brain, renal glomeruli and/or pulmonary capillaries leading to microinfarction and tissue hypoxia. DIC is also called consumptive coagulopathy, since excessive intravascular coagulation leads to consumption of platelets and nonenzymatic coagulation factors. The sequelae to excessive intravascular coagulation are systemic hemorrhagic diathesis due to thrombocytopenia, reduced quantities of coagulation factors and initiation of fibrinolysis. Initiation of fibrinolysis is caused by a plasminogen activator, which cleaves plasminogen bound to fibrin to plasmin. Plasmin degradates fibrin to FDPs, which can bind to fibrinogen receptors on platelets and prevent further platelet aggregation. In addition, thrombin binding to thrombomodulin results in activation of protein C, which cleaves and inactivates plasminogen activator inhibitor and coagulation factors V and VIII.
Finally, DIC is characterized by concurrent thrombocytopenia and depletion of coagulation factors and antiboagulants such as antithrombin III, protein C and protein S. The formation of fibrin within the microcirculation causes microangiopathic hemolytic anemia with schistozyte and keratocyte formation due to damaged membranes of erythrocytes.
Clinical features: DIC may present as acute, subacute or chronic disease. Whereas acute and subacute cases have clinical symptoms of multiorgan involvement such as respiratory signs (dyspnea, cyanosis), neurological signs (convulsions, coma), renal symptoms (oliguria, acute renal failure), chronic DIC usually causes only minor clinical signs or is subclinical. DIC is based on evaluation of blood parameters. Hemorrhagic diathesis predominates commonly in acute DIC and thrombotic complications are the main feature of subacute or chronic DIC. Acute DIC may develop primarily (e.g. caused by sepsis), or secondary to decompensation of chronic DIC. Acute DIC is often fatal with multiorgan failure and circulatory collapse.
Acute DIC is more commonly observed in dogs and is rare in cats.
Diagnosis: Diagnostics for DIC include concurrent prolongation of coagulation profiles (APTT, PT) and thrombocytopenia. In addition, there may be an increase in fibrin degradation products (FDPs), increase or decrease of fibrinogen, decreased antithrombin III, regenerative hemolytic anemia with schistocyte and keratocyte formation, neutrophilia with left shift or neutropenia and hypoalbuminemia. Increased FDPs may be observed in DIC, but is also seen in inflammatory diseases without concurrent DIC. Most commonly, fibrinogen is decreased in DIC; however, increased fibrinogen levels do not rule out DIC since fibrinogen is an acute phase protein synthesized in the liver and is often elevated in inflammatory conditions. Regenerative hemolytic anemia results from fibrin deposition in microcirculation and/or internal bleeding. Neutrophilia with left shift is a sequela to inflammation and/or marked tissue necrosis. Overwhelming inflammation may cause neutropenia. Inflammation may be the cause of DIC or develop secondarily in the course of DIC due to organ damage and immuno-suppression. Hypoalbuminemia may be a sequela to inflammation and/or excessive external bleeding.
-by Young Choi, ECFVG Student
-edited by Dr. Sandra Schoeniger, ADDL Graduate Student
References:
-
Pathologic Basis of Disease, 6th ed: 1999. Cotran RS, Kumar V and Collins T (eds) S.B. Saunders Co.
-
Veterinary Laboratory Medicine, 3rd ed): 1994. Duncan JR, Prasse KW and Mahaffey EA (eds). Iowa State University Press