Tumor types: There has been a long-lasting debate about classification of canine mammary tumors. According to the World Health Organization (WHO), canine mammary tumors are histologically classified into four categories: malignant tumors, benign tumors, unclassified tumors, and mammary hyperplasias/dysplasias. This classification reflects cellular atypia, pattern of neoplastic growth (e.g. tubulopapillary vs. solid), the origin of neoplastic cells (e.g. epithelial vs. mesenchymal), and descriptive morphology of each cellular component. Subclassification depends on clarification of neoplastic cell profile. The most common types are benign mixed tumor, adenoma, and adenocarcinoma. Benign mixed tumors consist of epithelial tumors and mesenchymal tumors, which can be manifested as bone, cartilage, or fibrous tumor.
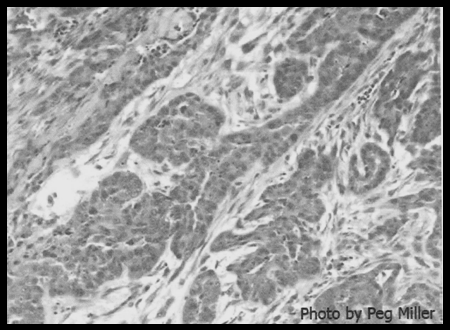
Adenoma and adenocarcinoma have many different subtypes. In order to incorporate prognostic factors, reclassification of canine mammary carcinoma has been attempted with statistical backups. This reclassification, in the order of increasing malignancy, includes non-infiltrating carcinoma, complex carcinoma (Figure 2), simple carcinoma and simple anaplastic carcinoma. |
It may also be of note that inflammatory carcinoma is not a distinct entity of mammary carcinoma, but rather, a particularly invasive mammary carcinoma with prominent inflammation. Inflammatory carcinomas account for less than 5% of all mammary tumors.
Causes and risk factors: The cause of canine mammary tumors is unknown; however, there are several factors that may influence the development of mammary gland tumors. That hormones such as estrogen and progesterone can be a risk factor is shown by the fact that ovariohysterectomy decreases the incidence of mammary tumors by avoiding the influence of these hormones. However, risk of developing a mammary tumor in later life is closely associated with the time when a bitch is spayed. If the dog is spayed before the first estrus, such risk is less than 1%. If the spay is done before the 2nd or 3rd estrus, the risk is 8% and 26%, respectively. Little benefit has been reported with spaying after the 3rd estrus. Obesity has been correlated with higher prevalence of mammary tumors in humans and dogs. Inherited predisposition for the development of mammary neoplasms has been described in human medicine, but studies are still underway in veterinary medicine.
Clinical signs: What will the pet owners notice?& Canine mammary tumor usually appears as variably-sized, single or multiple, soft to firm, discrete to poorly-defined masses or lumps associated with mammary gland(s). Dog owners may notice color change (red to purple) and/or ulceration on these masses. Clinical signs relevant to tumor-associated disease may be noticed on rare occasions. In particular, inflammatory carcinoma has been described to cause significant pain in the mammary region, axilla, groin, or medial aspects of the limbs due to extensive inflammation and/or edema secondary to tumor invasion in regional lymph vessels and nodes. With metastatic disease, clinical manifestations would reflect the affected organ’s location and function; for instance, a dog with pulmonary metastasis might show dyspnea or intolerance for exercise.
Diagnosis: Clinical evaluation of the patient is important as part of the diagnostic procedures. Thorough palpation of both mammary chains is indispensable. Tumors are more often found in the caudal pair of mammary glands. Multicentric involvement is common. Care should be taken to distinguish neoplastic from non-neoplastic masses such as cystic hyperplasia or duct ectasia if a patient is in estrus or has recently experienced pregnancy or pseudopregnancy. These masses sometimes simulate neoplasia; however, they usually regress as the& influence of estrogen declines.
As a part of the clinical evaluation, complete blood count and serum chemistry profiles are performed. Thoracic (3 views-left and right laterals and ventro- dorsal) and abdominal (2 views—lateral and ventro-dorsal) radiographs are useful to detect metastases. Ultrasound examination is indicated if metastasis to the abdominal organs is suspected.
The definitive diagnosis is based on histopathology on excisional biopsy specimens. In addition to aforementioned histological classification, WHO suggests tumor-node-metastasis (TNM) staging on canine mammary tumors to provide more practical prognostic information.
This staging is based on the size of the primary tumor, presence/absence of tumor metastasis to regional lymph nodes, and presence/absence of distant metastasis (Table 1). The greater the stage, the poorer the prognosis.
Stage
|
Primary
Tumor |
Regional LN Status |
Distant Metastasis |
I |
T1 |
NO |
MO |
II |
T2 |
NO |
MO |
III |
T3 |
NO |
MO |
IV |
Any T |
N1 |
MO |
V |
Any T |
Any N |
M1 |
Table 1. Modified TNM staging of canine mammary gland tumor.
- T1 < 3 cm maximum diameter
- T2 3-5 cm maximum diameter
- T3 > 5 cm maximum diameter
- NO Histologically no metastasis
- N1 Histologic metastasis
- MO No distant metastasis
- M1 Distant metastasis detected.
(Reference: Philbert JC et al: 2003.J Vet Intern Med 17:102-6)
Though fine needle aspirate (FNA) and cytological evaluation of the sample has been reported as part of the diagnostic workup, they rarely provide information as to the malignancy of a mammary tumor. Mast cell tumor in a mammary location can be readily ruled in/out by FNA.
Treatment: There are several options to treat canine mammary tumors including surgery, chemotherapy, radiation, immunotherapy, hormonal therapy, and diet. Nonetheless, surgical excision is still the most effective modality. The choice of surgical methods has been vigorously discussed; however, it is important to tailor the remedy to clients’ needs and to treat patients individually. If surgery is successful, with clear& histologic margins, and the patient has no evidence of lymph node involvement or metastasis, chemotherapy is not recommended. The most commonly used chemotherapeutic agents are doxorubicin and cisplatin. One potential side effect of doxorubicin is cardio-toxicity. Potential renal toxicity may occur with the use of cisplatin. Paclitaxel has been experimentally used to treat canine malignant mammary tumors with high incidence of side effects. Hormonal therapy, such as tamoxifen citrate (an antiestrogen drug used in human estrogen receptor-positive breast cancer), has been used in a limited number of dogs. An advantage of this medication is that it can be given orally. The disadvantage is that 25% of the animals have side effects such as vulvar swelling and pyometra. Radiation therapy and immunotherapy have been studied, but efficacy is not proven. A theory proposing that a high protein/low fat diet may prolong survival has been advanced.
Prognosis: The most important prognostic information is derived from the WHO staging system and histologic diagnosis. Size of the tumor is thought to be a good prognostic indicator. Dogs with smaller (less than 5 cm in diameter) malignant tumors have a better prognosis for long-term survival. Metastasis is observed in about half of malignant tumor cases. Histologic evaluation is critical not only to determine the origin of the neoplastic cells, but also to find microscopic evidence of possible metastases. For example, invasiveness of tumor cells into adjacent normal tissue can be demonstrated by immunohistochemistry with antibody for calponin (marker for myoepithelial cells), which will distinguish in situ from invasive carcinoma. Early surgical intervention and the method of surgery play important roles in prolonging survival. Ovariohysterectomy at the time of tumor excision has been recognized to increase survival time.
-by Dr. Ikki Mitsui, ADDL Graduate Student
References
-
Alenza MDP, Tabanera E, Peňa: 2001. Inflammatory mammary carcinoma in dogs: 33 cases (1995-1999). JAVMA 219:1110-1114.
-
Hahn KA, Richardson RC, Knapp DW: 1992. Canine malignant mammary neoplasia: biological behavior, diagnosis and treatment alternatives. J Am Anim Hosp Assoc 28:251-56.
-
Misdorp W: 2002. Tumors of the mammary gland. IN: Tumors in Domestic Animals, ed. Meuten DJ, 4th ed. pp 575-606. Iowa State Press, Ames, IA
-
Philibert JC, Snyder PW, Glickman N, Glickman LT, Knapp DW, Waters DJ: 2003. Influence of host factors on survival in dogs with malignant mammary gland tumors. J Vet Intern Med 17: 102-106.
-
Rutteman GR, Withrow SJ, MacEwen EG: 2001. Tumors of the mammary gland. IN: Small Animal Clinical Oncology, eds. Withrow SJ, MacEwen EG, 3rd ed., pp 455-477. WB Saunders, Philadelphia
-
Waldron DR: 2001. Diagnosis and surgical management of mammary neoplasia in dogs and cats. Vet Med 96: 943-948
|